What is diffuse large B-cell lymphoma (DLBCL)?
Diffuse large B-cell lymphoma is the most common type of non-Hodgkin’s lymphoma, accounting for 30% of all non-Hodgkin’s lymphomas. It is diagnosed in around 3,000 new people each year in Spain. It is an aggressive type B lymphoma (fast-growing). Its incidence is 50-60 new cases per million inhabitants per year and increases with age.
Although it is seen at any age, the median age of patients with large cell lymphoma is 60-65 years. Due to advances in the diagnosis of neoplastic diseases using techniques for the study of genes involved in the origin of lymphomas, it has been possible to identify subtypes within this category with different prognoses.
There are two main subtypes: diffuse germinal centre lymphoma and activated B-cell lymphoma.
The causes of DLBCL are unknown, as in most lymphomas, and the most common symptom is the appearance of an enlarged lymph node (see general section on NHL). Another reason for consultation may be a persistent dry cough with a chest X-ray finding of a mass in the mediastinum (the region between the two lungs). In 30% of cases the patient presents with so-called B-symptoms (weight loss of more than 10% in the last six months without cause, evening fever and night sweats) as well as fatigue.
In about one third of patients, DLBCL initially affects organs outside the lymphatic system. The most common are in the gastrointestinal tract, with the main location being the stomach, although they can range from the salivary glands and tonsils to the large intestine. These tumours can cause pain and obstruction to normal gastrointestinal transit, but can also cause ulcers and digestive haemorrhages. Extranodal lymphomas can appear in any organ or site of the human body.
Histological study of the lymph node must always be completed with an immunohistochemical, cytogenetic and molecular study in order to have a perfect typing of the lymphoma and to make a correct differential diagnosis with other similar lymphomas. It is important to rule out chromosomal alterations typical of other types of lymphomas such as t(14,18) typical of follicular lymphoma (although both types of lymphoma are frequently associated), or t(11,14) typical of mantle lymphoma. Ki-67 staining of the biopsy specimen is useful to assess the proliferative activity of this type of tumour.
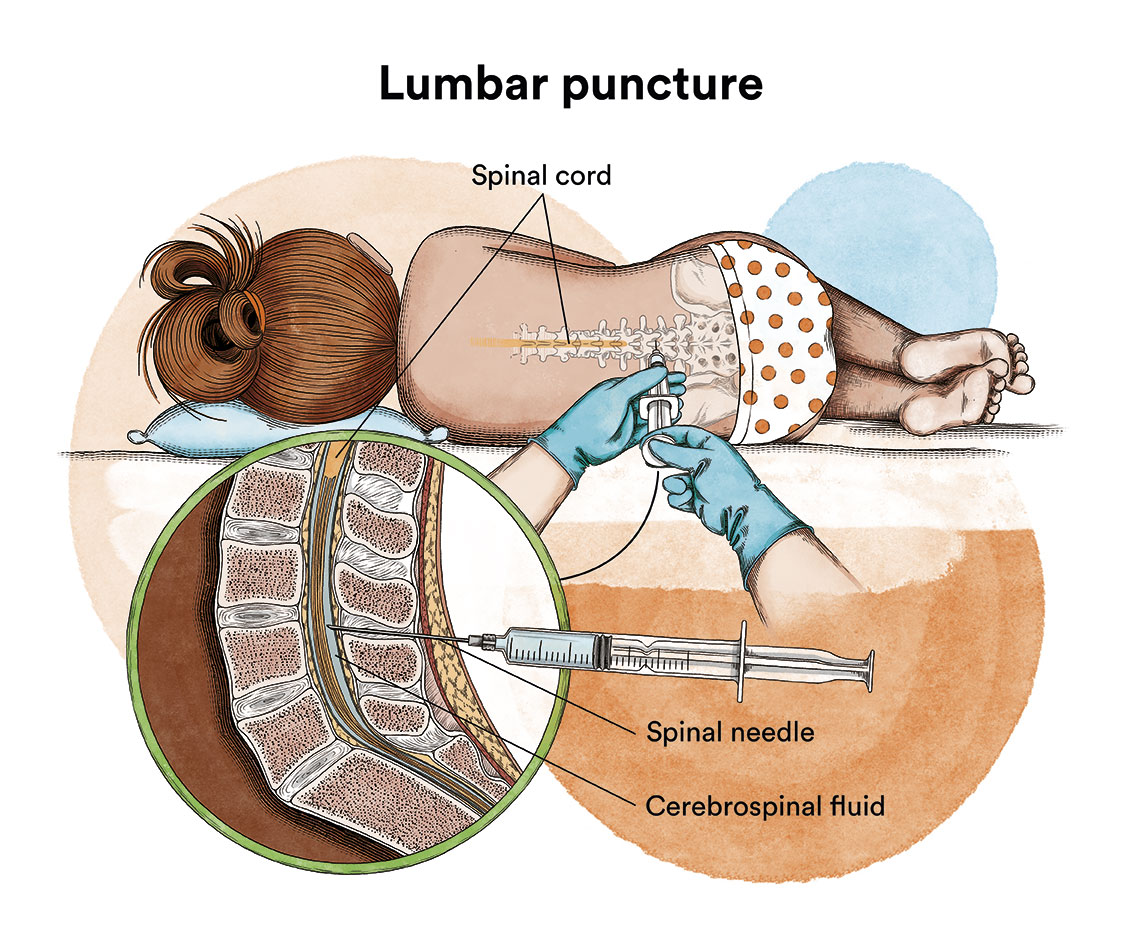
In the extension study (see general section on NHL), in addition to the tests mentioned above, a lumbar puncture (flow cytometry +/- cytology) should be considered: indicated in patients with a high risk of CNS involvement such as those with testicular, breast, renal or epidural involvement or when there is more than one extranodal location and very high LDH.
In DLBCL, a prognostic score called IPI is applied, which is complementary to the lymphoma stage and is based on the following risk factors: patient age, extranodal involvement, stage, LDH and general condition of the patient.

What is the treatment for diffuse large B-cell lymphoma?
The treatment of choice for DLBCL is chemotherapy associated with radiotherapy (on localised or large affected areas), as it is a type of lymphoma that tends to grow rapidly.

The most commonly used chemotherapy regimen at present is R-CHOP, which combines rituximab with cyclophosphamide, adriamycin, vincristine and prednisone, with a variable frequency of administration and number of cycles depending on each case. Radiotherapy can be effective in treating localised affected areas. The haematopoietic stem cell transplantation (usually autogenic and more rarely allogeneic) is limited to patients refractory to first-line treatment or relapsed, as long as the disease remains chemosensitive. In specific cases where there is a risk of central nervous system infiltration, the administration of intrathecal chemotherapy (injected directly into the cerebrospinal fluid via lumbar puncture) or the use of high doses of methotrexate intravenously, as this drug can also reach the cerebrospinal fluid, should be considered with each cycle.
In stage I and II DLBCL, R-CHOP chemotherapy is often given for 3-6 cycles repeated every 3 weeks, which may be followed by radiotherapy to the affected lymph node areas. In stages III and IV, at least 6 cycles of R-CHOP will be given as first-line treatment. Different ways have been investigated to improve the efficacy of the CHOP chemotherapy regimen in higher risk patients by escalating the doses, adopting other drugs or shortening the interval between cycles.
There is a specific subgroup of DLBCL with its own entity, the primary mediastinal lymphoma, which is characterised, as the name suggests, by a mediastinal mass (located between the lungs) usually of large dimensions. The reason for consultation is usually persistent cough or a more striking and severe picture called superior vena cava syndrome, characterised by oedema and swelling of the entire face, neck and upper chest, respiratory symptoms, difficulty in swallowing, all secondary to compression of the superior vena cava. A more intensive regimen called DA-EPOCH containing rituximab, etopoxide, adriamycin, vincristine, cyclophosphamide and prednisone is frequently used in this lymphoma.
Another subgroup characterised by their aggressiveness and poor response to conventional treatments are the double or triple hit lymphomas, so called because of the presence of specific markers (c-myc, bcl2 and/or bcl 6 rearrangement). In this case, intrathecal prophylaxis is indicated.
In case of relapse or refractoriness to first-line treatment, the most commonly used regimens are DHAP (dexamethasone, cytarabine and cisplatin), ESHAP (etoposide, methylprednisolone, cytarabine and cisplatin) or ICE (ifosfamide, carboplatin and etoposide).
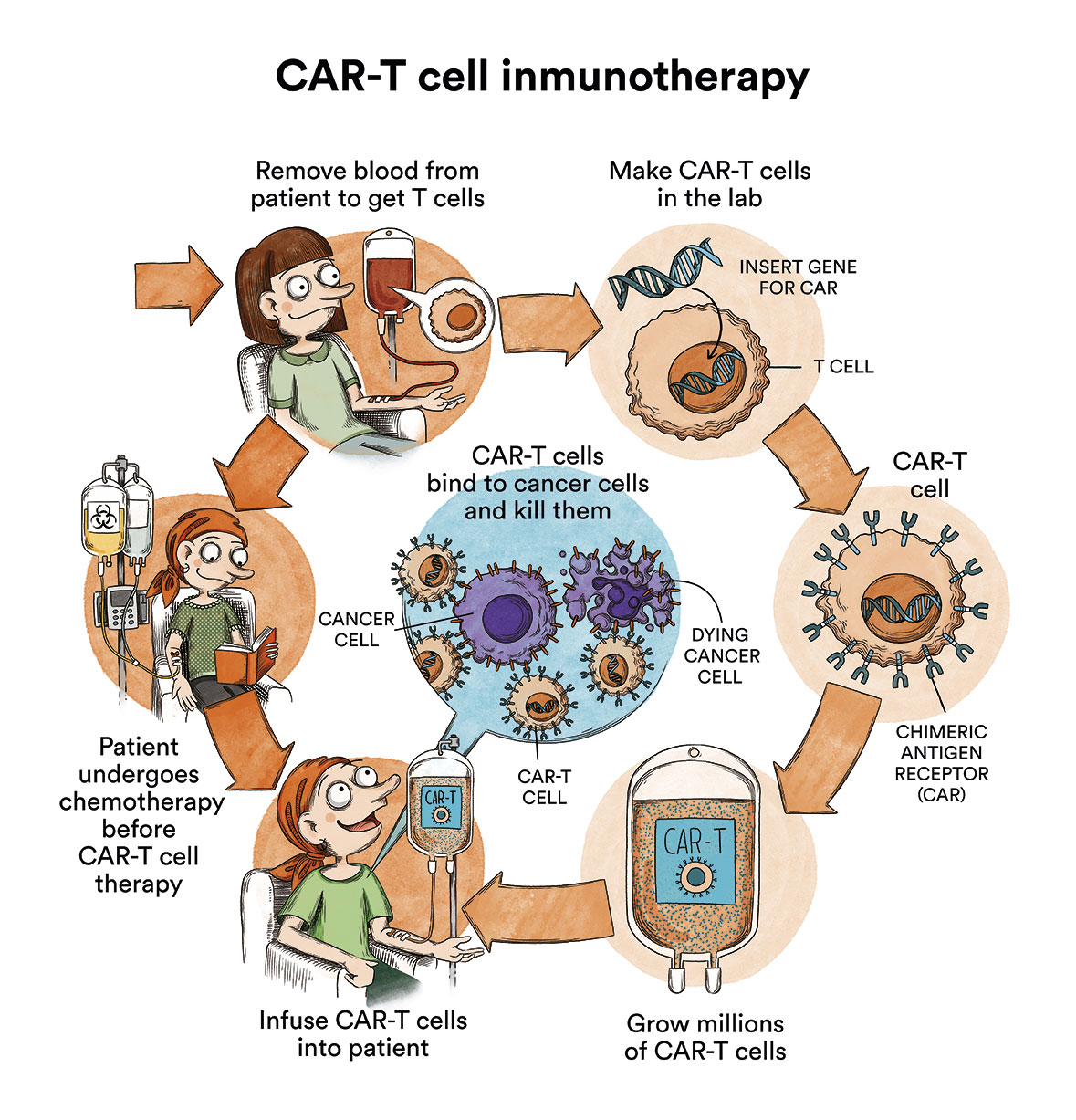
The blood stem cell transplantation, specifically autologous, may be indicated a posteriori in young patients (<70 years) with an increased risk of lymphoma relapse, such as those refractory to first-line treatment or who have relapsed after first-line treatment, and provided that the disease remains chemosensitive. However, with the advent of immunotherapy, especially CART therapy (content in spanish), the indication for transplantation is beginning to be questioned, especially beyond the second line, and the indication for allogeneic transplantation, which was classically offered in patients who relapsed after autologous transplantation, is becoming less frequent.
CART therapy, targeting CD19, a common lymphomatous cell marker, is now an established indication in adult DLBCL in the following situations:
- Primary refractoriness after 2 previous lines of treatment
- First relapse without response, or beyond the second relapse
- Relapse after previous autologous transplantation
The administration of CART therapy is only performed in national third level centres that have been authorised by the Ministry of Health, and each case must be assessed and approved by a national committee of experts. On the other hand, there are immunotherapy alternatives with monoclonal antibodies, which also target specific markers such as CD19, or 2 different markers, and are usually administered within clinical trials. In summary, the treatment scenario for DLBCL, beyond the standard first-line chemotherapy treatment, is currently under review, pending confirmation of the promising results of immunotherapy.

What are the chances of patients with diffuse large B-cell lymphoma being cured?
Up to 80% of young patients can be cured with this therapeutic approach, with this probability decreasing with increasing age. The “germinal centre” type has better prognosis and survival with standard treatments and clearly benefits from the addition of rituximab to treatment, which is not as evident with the “activated B-cell” type, which has a worse prognosis. However, with the new immunotherapy strategies described above, especially CART therapy, a radical change in the overall scenario and prognosis of this disease is expected.
Links of interest concerning medical issues relating to diffuse large B-cell lymphoma
Diffuse large B-cell lymphoma (DLBCL). Blood Cancer UK
Diffuse large B cell lymphoma. Cancer Research UK
Diffuse large B-cell lymphoma (DLBCL). Macmillan Cancer Support
Links of interest on other topics related to non-Hodgkin’s lymphoma:
TESTIMONIAL MATERIALS
You can order the booklets in paper format for free delivery in Spain by e-mail: imparables@fcarreras.es
BONE MARROW TRANSPLANT
- Bone Marrow Transplant Guide. Josep Carreras Foundation (content in Spanish)
- What is HLA and how does it work? Josep Carreras Foundation (content in Spanish)
- Graft-versus-Host Disease. Josep Carreras Foundation (content in Spanish)
- History of Bone Marrow Transplantation. Josep Carreras Foundation (content in Spanish)
- How is the search for an anonymous donor conducted? Josep Carreras Foundation (content in Spanish)
FOOD
- How to maintain a healthy diet during treatment? Josep Carreras Foundation (content in Spanish)
- Nutrition guide. Leukemia & Lymphoma Society
OTHER
- Ideas on what to take with me to the isolation chamber. Josep Carreras Leukaemia Foundation (content in Spanish)
- Travel tips for people with cancer. Josep Carreras Leukaemia Foundation (content in Spanish)
- Physiotherapy manual for haematological and transplant patients. Josep Carreras Leukaemia Foundation (content in Spanish)
- Prevention and treatment of oral mucositis. Josep Carreras Leukaemia Foundation (content in Spanish)
- Oral hygiene in oncohaematological patients. Josep Carreras Leukaemia Foundation (content in Spanish)
- Fertility manual: Suffering from blood cancer and becoming a parent. Josep Carreras Leukaemia Foundation (content in Spanish)
- Skin care in the oncohaematological patient. Josep Carreras Leukaemia Foundation (content in Spanish)
- Aesthetic Oncology Manual. Josep Carreras Leukaemia Foundation (content in Spanish)
- Leukaemia and sexuality. Josep Carreras Leukaemia Foundation (content in Spanish)
- 7 ways to wear a scarf. Josep Carreras Leukaemia Foundation (content in Spanish)
Links of interest: local/provincial or state entities that can provide you with resources and services specialised in leukaemia, lymphoma or cancer patients:
In Spain there is a large network of associations for haematological cancer patients which, in many cases, can provide information, advice and even carry out certain procedures. These are the contacts of some of them by Autonomous Community:
All these organisations are external to the Josep Carreras Foundation.
STATE
- AMILO (Asociación Española de Amiloidosis)
- ACLIF (Asociación para la cura del linfoma folicular)
- AEAL (ASOCIACIÓN ESPAÑOLA DE AFECTADOS POR LINFOMA, MIELOMA y LEUCEMIA)
- AECC (ASOCIACIÓN ESPAÑOLA CONTRA EL CÁNCER). Present in the different provinces and in many municipalities. Contact the nearest branch or call 900 100 036 (24h).
- AELCLES (Agrupación Española contra la Leucemia y Enfermedades de la Sangre)
- CEMMP (Comunidad Española de Pacientes de Mieloma Múltiple)
- JOSEP CARRERAS LEUKAEMIA FOUNDATION
- FUNDACIÓN SANDRA IBARRA
- GEPAC (GRUPO ESPAÑOL DE PACIENTES CON CÁNCER)
- MPN España (Asociación de Afectados Por Neoplasias Mieloproliferativas Crónicas)
ANDALUCÍA
- AECC (ASOCIACIÓN ESPAÑOLA CONTRA EL CÁNCER). Present in the different provinces and in many municipalities. Contact the nearest branch.
- ALUSVI (ASOCIACIÓN LUCHA Y SONRÍE POR LA VIDA). Sevilla
- APOLEU (ASOCIACIÓN DE APOYO A PACIENTES Y FAMILIARES DE LEUCEMIA). Cádiz
ARAGÓN
- AECC (ASOCIACIÓN ESPAÑOLA CONTRA EL CÁNCER). Present in the different provinces and in many municipalities. Contact the nearest branch.
- ASPHER (ASOCIACIÓN DE PACIENTES DE ENFERMEDADES HEMATOLÓGICAS RARAS DE ARAGÓN)
- DONA MÉDULA ARAGÓN
ASTURIAS
- AECC (ASOCIACIÓN ESPAÑOLA CONTRA EL CÁNCER). Present in the different provinces and in many municipalities. Contact the nearest branch.
- ASTHEHA (ASOCIACIÓN DE TRASPLANTADOS HEMATOPOYÉTICOS Y ENFERMOS HEMATOLÓGICOS DE ASTURIAS)
CANTABRIA
- AECC (ASOCIACIÓN ESPAÑOLA CONTRA EL CÁNCER). Present in the different provinces and in many municipalities. Contact the nearest branch.
CASTILLA LA MANCHA
- AECC (ASOCIACIÓN ESPAÑOLA CONTRA EL CÁNCER). Present in the different provinces and in many municipalities. Contact the nearest branch.
CASTILLA LEÓN
- ABACES (ASOCIACIÓN BERCIANA DE AYUDA CONTRA LAS ENFERMEDADES DE LA SANGRE)
- AECC (ASOCIACIÓN ESPAÑOLA CONTRA EL CÁNCER). Present in the different provinces and in many municipalities. Contact the nearest branch.
- ALCLES (ASOCIACIÓN LEONESA CON LAS ENFERMEDADES DE LA SANGRE). León.
- ASCOL (ASOCIACIÓN CONTRA LA LEUCEMIA Y ENFERMEDADES DE LA SANGRE). Salamanca.
CATALUÑA
- ASSOCIACIÓ FÈNIX. Solsona
- FECEC (FEDERACIÓ CATALANA D’ENTITATS CONTRA EL CÁNCER
- FUNDACIÓ KÁLIDA. Barcelona
- FUNDACIÓ ROSES CONTRA EL CÀNCER. Roses
- LLIGA CONTRA EL CÀNCER COMARQUES DE TARRAGONA I TERRES DE L’EBRE. Tarragona
- MielomaCAT
- ONCOLLIGA BARCELONA. Barcelona
- ONCOLLIGA GIRONA. Girona
- ONCOLLIGA COMARQUES DE LLEIDA. Lleida
- ONCOVALLÈS. Vallès Oriental
- OSONA CONTRA EL CÀNCER. Osona
- SUPORT I COMPANYIA. Barcelona
- VILASSAR DE DALT CONTRA EL CÀNCER. Vilassar de Dalt
VALENCIAN COMMUNITY
- AECC (ASOCIACIÓN ESPAÑOLA CONTRA EL CÁNCER). Present in the different provinces and in many municipalities. Contact the nearest branch.
- ASLEUVAL (ASOCIACIÓN DE PACIENTES DE LEUCEMIA, LINFOMA, MIELOMA Y OTRAS ENFERMEDADES DE LA SANGRE DE VALENCIA)
EXTREMADURA
- AECC (ASOCIACIÓN ESPAÑOLA CONTRA EL CÁNCER). Present in the different provinces and in many municipalities. Contact the nearest branch.
- AFAL (AYUDA A FAMILIAS AFECTADAS DE LEUCEMIAS, LINFOMAS; MIELOMAS Y APLASIAS)
- AOEX (ASOCIACIÓN ONCOLÓGICA EXTREMEÑA)
GALICIA
- AECC (ASOCIACIÓN ESPAÑOLA CONTRA EL CÁNCER). Present in the different provinces and in many municipalities. Contact the nearest branch.
- ASOTRAME (ASOCIACIÓN GALLEGA DE AFECTADOS POR TRASPLANTES MEDULARES)
BALEARIC ISLANDS
- ADAA (ASSOCIACIÓ D’AJUDA A L’ACOMPANYAMENT DEL MALALT DE LES ILLES BALEARS)
- AECC (ASOCIACIÓN ESPAÑOLA CONTRA EL CÁNCER). Present in the different provinces and in many municipalities. Contact the nearest branch.
CANARY ISLANDS
- AECC (ASOCIACIÓN ESPAÑOLA CONTRA EL CÁNCER). Present in the different provinces and in many municipalities. Contact the nearest branch.
- AFOL (ASOCIACIÓN DE FAMILIAS ONCOHEMATOLÓGICAS DE LANZAROTE)
- FUNDACIÓN ALEJANDRO DA SILVA
LA RIOJA
- AECC (ASOCIACIÓN ESPAÑOLA CONTRA EL CÁNCER). Present in the different provinces and in many municipalities. Contact the nearest branch.
MADRID
- AECC (ASOCIACIÓN ESPAÑOLA CONTRA EL CÁNCER). Present in the different provinces and in many municipalities. Contact the nearest branch.
- AEAL (ASOCIACIÓN ESPAÑOLA DE LEUCEMIA Y LINFOMA)
- CRIS CONTRA EL CÁNCER
- FUNDACIÓN LEUCEMIA Y LINFOMA
MURCIA
- AECC (ASOCIACIÓN ESPAÑOLA CONTRA EL CÁNCER). Present in the different provinces and in many municipalities. Contact the nearest branch.
NAVARRA
- AECC (ASOCIACIÓN ESPAÑOLA CONTRA EL CÁNCER). Present in the different provinces and in many municipalities. Contact the nearest branch.
BASQUE COUNTRY
- AECC (ASOCIACIÓN ESPAÑOLA CONTRA EL CÁNCER). Present in the different provinces and in many municipalities. Contact the nearest branch.
- PAUSOZ-PAUSO. Bilbao
AUTONOMOUS CITIES OF CEUTA AND MELILLA
- AECC CEUTA (ASOCIACIÓN ESPAÑOLA CONTRA EL CÁNCER)
- AECC MELILLA (ASOCIACIÓN ESPAÑOLA CONTRA EL CÁNCER)
Support and assistance
We also invite you to follow us through our main social media (Facebook, Twitter and Instagram) where we often share testimonies of overcoming this disease.
If you live in Spain, you can also contact us by sending an e-mail to imparables@fcarreras.es so that we can help you get in touch with other people who have overcome this disease.