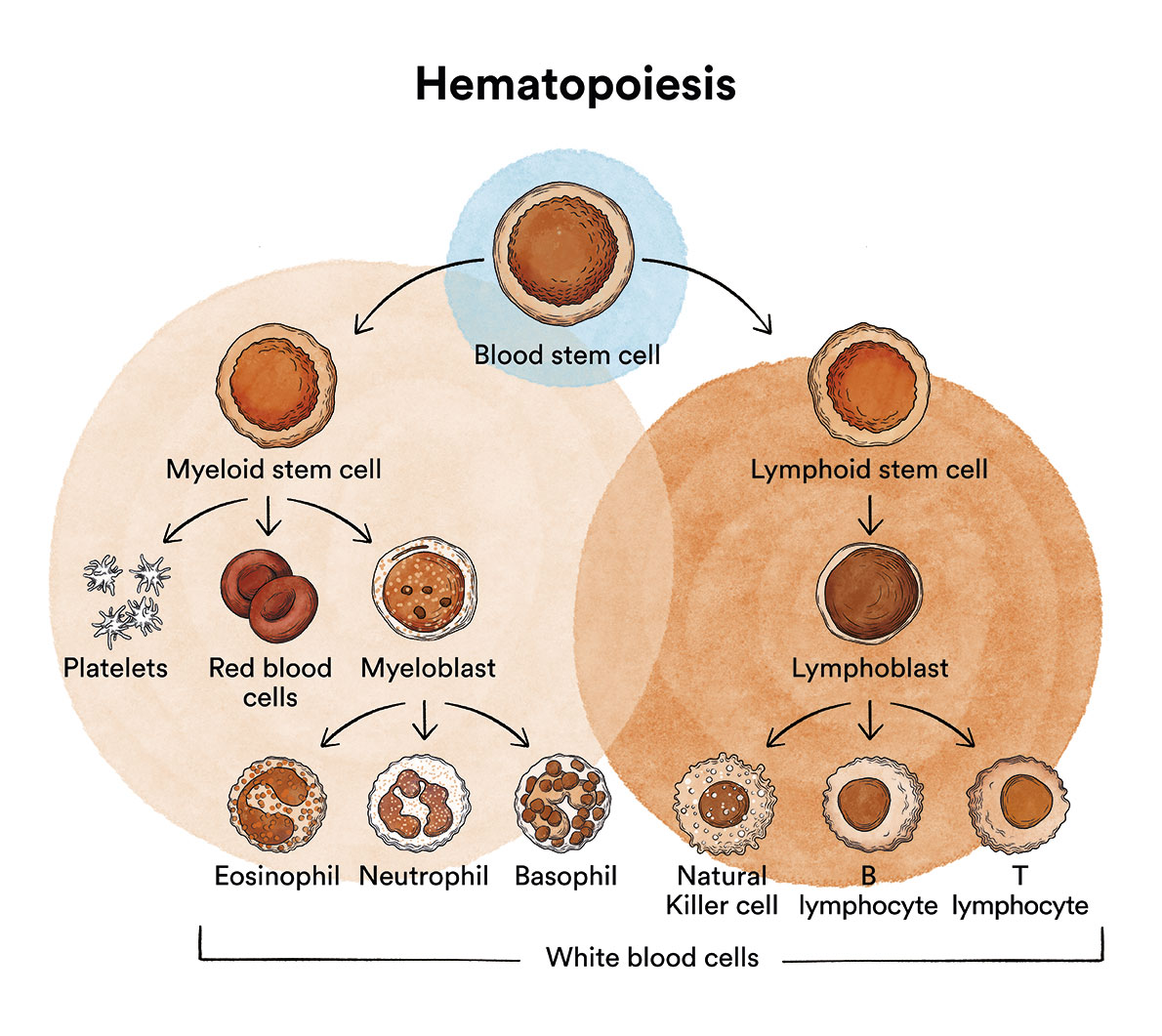
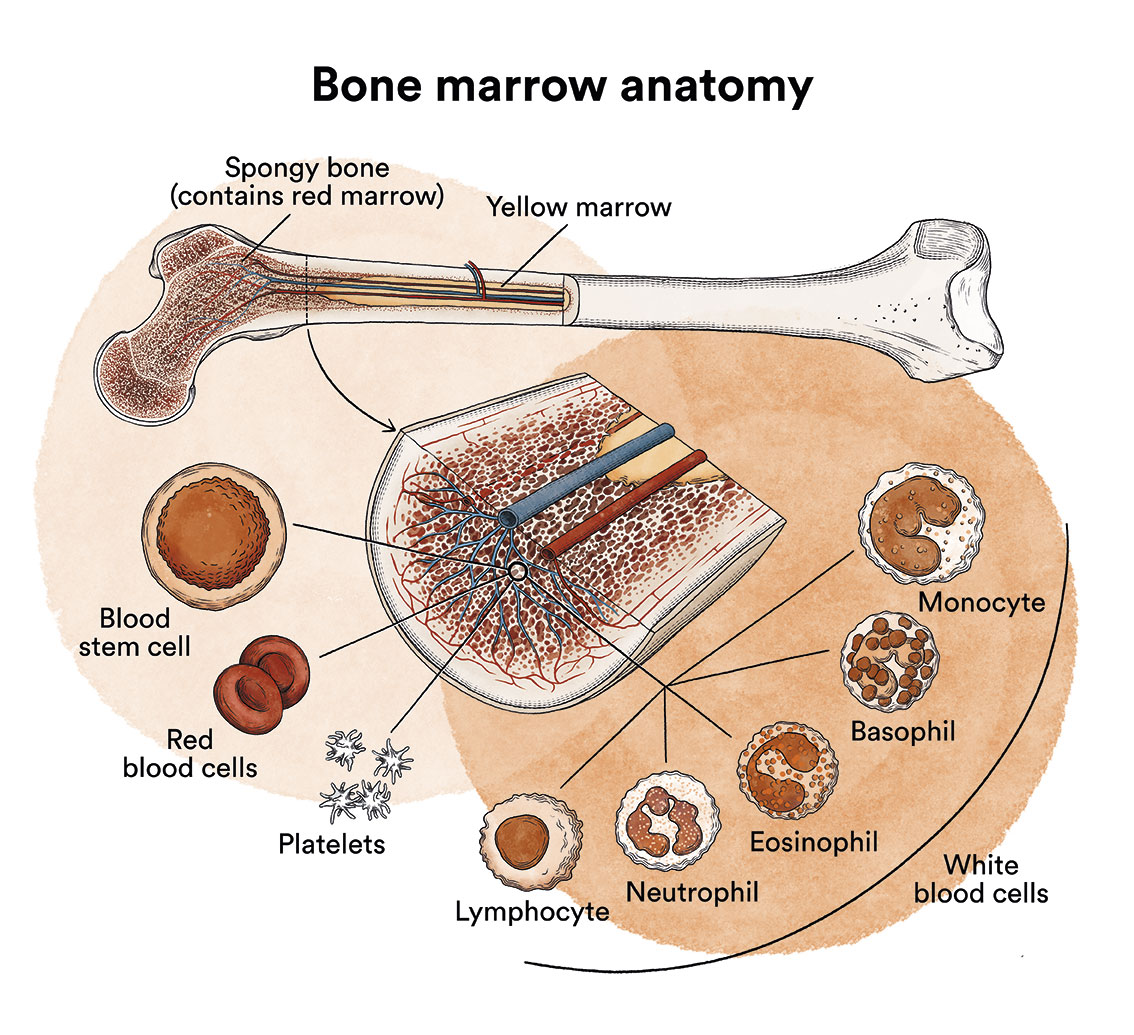
How does bone marrow work and what are the types of blood cells?
Primary amyloidosis is a disease originating in the bone marrow, classified within the group of monoclonal gammopathies.
See section Leukaemia, bone marrow and blood cells.
What is primary amyloidosis and who does it affect?
Primary amyloidosis is a disease classified within the group of monoclonal gammopathies. This is a type of cancer in which fibrillar proteins (amyloid substance) are deposited in tissues in sufficient quantities to impair the normal function of the affected organ.
The causes of the production of the amyloid substance and its deposition in tissues are unknown, although primary amyloidosis is related to abnormal production of antibodies by B-lymphocyte-derived cells, the plasma cells.
Primary amyloidosis is a very rare type of neoplasm. Its incidence in Spain is around 9 cases per million inhabitants per year. It tends to affect predominantly older men, with the average age being 65 years.
What are the causes of primary amyloidosis?
There is no known direct causative factor for the onset of primary amyloidosis. It is not a contagious disease.
What are the symptoms of primary amyloidosis?
Primary amyloidosis usually has a chronic course and a very slow progression and may remain asymptomatic for years, requiring no treatment.
The main symptoms, once clinically manifested, are tiredness and weight loss, oedema (due to kidney involvement causing nephrotic syndrome in which excessive amounts of protein are lost in the urine), dyspnoea (shortness of breath due to heart failure), enlargement of the liver (hepatomegaly), sensory disorders in the hands and feet (neuropathy), enlargement of the tongue, tendency to hypotension, diarrhoea, impotence, among others. These clinical manifestations are due to organ dysfunction caused by deposits of amyloid material.
How is primary amyloidosis diagnosed?
 The diagnosis of primary amyloidosis is based on the finding of amyloid material in the tissues (by Congo red staining). Blood tests are usually performed, in addition to a biopsy of the abdominal subcutaneous fat (positive in 80% of patients with amyloidosis) and bone marrow (sensitivity of 60-70%). If this biopsy is negative, another rectal or minor salivary gland biopsy would be performed and, if the results are still negative, a biopsy of an affected organ (kidney, endo-myocardium, nerve, liver) depending on the suspicion.
The diagnosis of primary amyloidosis is based on the finding of amyloid material in the tissues (by Congo red staining). Blood tests are usually performed, in addition to a biopsy of the abdominal subcutaneous fat (positive in 80% of patients with amyloidosis) and bone marrow (sensitivity of 60-70%). If this biopsy is negative, another rectal or minor salivary gland biopsy would be performed and, if the results are still negative, a biopsy of an affected organ (kidney, endo-myocardium, nerve, liver) depending on the suspicion.
The most common systemic amyloidosis is light chain or AL amyloidosis (74% of systemic amyloidoses), caused by monoclonal light chain fragments usually produced by a small clone of B-cells, and in about 80% of cases the light chain is lambda. However, other less common forms of amyloidosis, such as familial, secondary and senile amyloidosis, with a specific amyloid substance must be ruled out.
It is important, both at diagnosis and during follow-up, to rule out possible organ involvement by amyloid fibrils through clinical history, as well as by determination of biomarkers of cardiac involvement (BNP/proBNP and troponin), together with imaging tests such as echocardiography and cardiac MRI if there are cardiac symptoms, renal (quantification of proteinuria, albuminuria, in 24-hour urine) and serum free light chain ratio, in order to be able to obtain a pre-symptomatic diagnosis. Early diagnosis is key to improving the prognosis of patients with amyloidosis.
What is the treatment for primary amyloidosis?
 The European Commission has approved daratumumab SC in combination with bortezomib, cyclophosphamide and dexamethasone (D-VCd) for the treatment of adult patients with newly diagnosed systemic light chain amyloidosis. This approval makes this daratumumab-based regimen the first approved treatment for AL amyloidosis in Europe. Participation in clinical trials is a priority whenever available.
The European Commission has approved daratumumab SC in combination with bortezomib, cyclophosphamide and dexamethasone (D-VCd) for the treatment of adult patients with newly diagnosed systemic light chain amyloidosis. This approval makes this daratumumab-based regimen the first approved treatment for AL amyloidosis in Europe. Participation in clinical trials is a priority whenever available.
In parallel, it should be assessed whether the patient is eligible (due to age and organ damage) for an autologous haematopoietic stem cell transplant. In eligible patients, the toxicity of the procedure is acceptable and transplantation can be considered as a first-line therapeutic option or preceded by treatment. Although transplantation can be performed without pre-treatment, pre-transplant induction is often recommended if plasma cell infiltration in the bone marrow > 10% or if delayed transplantation is anticipated. Similarly, patients who are not initially candidates for transplantation may be candidates for transplantation after 2-3 cycles of treatment.
It must be borne in mind that, unfortunately, transplantation does not cure the disease, but it does allow for achieving remissions, sometimes prolonged, and improvement of the affected organs.
In selected cases where cardiac damage is the main limiting factor, cardiac transplantation may be considered followed shortly after by haematopoietic transplantation. It is also not uncommon for the patient to need a kidney transplant, usually following autologous transplantation.
In cases that are not candidates for transplantation (due to little or excessive involvement) treatment is based on the previously mentioned D-VCd scheme, or variants such as CyBorDex (cyclophosphamide, bortezomib and dexamethasone), and BMDex (bortezomib, melphalan dexamethasone). In frailer patients, regimens are reduced to melphalan or cyclophosphamide and dexamethasone, or daratumomab monotherapy as an alternative.
Treatment also includes those specific to visceral involvement such as renal or cardiac failure.
The aim of all treatments is always to slow down the progression of the disease and improve the symptoms as, unfortunately, none of them can cure it.
What is the prognosis for patients with primary amyloidosis?
The prognosis for patients with primary amyloidosis depends largely on the organs affected. However, the absence of a treatment capable of slowing down the deposition and reversing the substance already deposited, and the usual advanced age of the patients, make their prognosis unfavourable.
Links of interest concerning medical issues relating to primary amyloidosis
AL Amyloidosis (Primary Amyloidosis). Cleveland Clinic
Links of interest on other topics related to Primary amyloidosis
TESTIMONIAL MATERIALS
You can order the booklets in paper format for free delivery in Spain by e-mail: imparables@fcarreras.es
BONE MARROW TRANSPLANT
- Bone Marrow Transplant Guide. Josep Carreras Foundation (content in Spanish)
- What is HLA and how does it work? Josep Carreras Foundation (content in Spanish)
- Graft-versus-Host Disease. Josep Carreras Foundation (content in Spanish)
- History of Bone Marrow Transplantation. Josep Carreras Foundation (content in Spanish)
- How is the search for an anonymous donor conducted? Josep Carreras Foundation (content in Spanish)
FOOD
- How to maintain a healthy diet during treatment? Josep Carreras Foundation (content in Spanish)
- Nutrition guide. Leukemia & Lymphoma Society
OTHER
- Ideas on what to take with me to the isolation chamber. Josep Carreras Leukaemia Foundation (content in Spanish)
- Travel tips for people with cancer. Josep Carreras Leukaemia Foundation (content in Spanish)
- Physiotherapy manual for haematological and transplant patients. Josep Carreras Leukaemia Foundation (content in Spanish)
- Prevention and treatment of oral mucositis. Josep Carreras Leukaemia Foundation (content in Spanish)
- Oral hygiene in oncohaematological patients. Josep Carreras Leukaemia Foundation (content in Spanish)
- Fertility manual: Suffering from blood cancer and becoming a parent. Josep Carreras Leukaemia Foundation (content in Spanish)
- Skin care in the oncohaematological patient. Josep Carreras Leukaemia Foundation (content in Spanish)
- Aesthetic Oncology Manual. Josep Carreras Leukaemia Foundation (content in Spanish)
- Leukaemia and sexuality. Josep Carreras Leukaemia Foundation (content in Spanish)
- 7 ways to wear a scarf. Josep Carreras Leukaemia Foundation (content in Spanish)
Links of interest: local/provincial or state entities that can provide you with resources and services specialised in leukaemia or cancer patients:
In Spain there is a large network of associations for haematological cancer patients that, in many cases, can inform you, advise you and even carry out certain procedures. These are the contacts of some of them by Autonomous Communities:
All these organisations are external to the Josep Carreras Foundation.
STATE
- AMILO (Asociación Española de Amiloidosis)
- CEMMP (Comunidad Española de Pacientes de Mieloma Múltiple)
- AEAL (ASOCIACIÓN ESPAÑOLA DE AFECTADOS POR LINFOMA, MIELOMA y LEUCEMIA)
- AECC (ASOCIACIÓN ESPAÑOLA CONTRA EL CÁNCER). Present is the different provinces and in many municipalities. Contact with the nearest branch or call 900 100 036 (24h).
- AELCLES (Agrupación Española contra la Leucemia y Enfermedades de la Sangre)
- Josep Carreras Leukaemia Foundation
- FUNDACIÓN SANDRA IBARRA
- GEPAC (GRUPO ESPAÑOL DE PACIENTES CON CÁNCER)
- MPN España (Asociación de Afectados Por Neoplasias Mieloproliferativas Crónicas)
ANDALUCÍA
- AECC (ASOCIACIÓN ESPAÑOLA CONTRA EL CÁNCER). Present is the different provinces and in many municipalities. Contact the nearest branch.
- ALUSVI (ASOCIACIÓN LUCHA Y SONRÍE POR LA VIDA). Sevilla
- APOLEU (ASOCIACIÓN DE APOYO A PACIENTES Y FAMILIARES DE LEUCEMIA). Cádiz
ARAGÓN
- AECC (ASOCIACIÓN ESPAÑOLA CONTRA EL CÁNCER). Present is the different provinces and in many municipalities. Contact the nearest branch.
- ASPHER (ASOCIACIÓN DE PACIENTES DE ENFERMEDADES HEMATOLÓGICAS RARAS DE ARAGÓN)
- DONA MÉDULA ARAGÓN
ASTURIAS
- AECC (ASOCIACIÓN ESPAÑOLA CONTRA EL CÁNCER). Present is the different provinces and in many municipalities. Contact the nearest branch.
- ASTHEHA (ASOCIACIÓN DE TRASPLANTADOS HEMATOPOYÉTICOS Y ENFERMOS HEMATOLÓGICOS DE ASTURIAS)
CANTABRIA
- AECC (ASOCIACIÓN ESPAÑOLA CONTRA EL CÁNCER). Present is the different provinces and in many municipalities. Contact the nearest branch.
CASTILLA LA MANCHA
- AECC (ASOCIACIÓN ESPAÑOLA CONTRA EL CÁNCER). Present is the different provinces and in many municipalities. Contact the nearest branch.
CASTILLA LEÓN
- ABACES (ASOCIACIÓN BERCIANA DE AYUDA CONTRA LAS ENFERMEDADES DE LA SANGRE)
- AECC (ASOCIACIÓN ESPAÑOLA CONTRA EL CÁNCER). Present is the different provinces and in many municipalities. Contact the nearest branch.
- ALCLES (ASOCIACIÓN LEONESA CON LAS ENFERMEDADES DE LA SANGRE). León.
- ASCOL (ASOCIACIÓN CONTRA LA LEUCEMIA Y ENFERMEDADES DE LA SANGRE). Salamanca.
CATALUÑA
- ASSOCIACIÓ FÈNIX. Solsona
- FECEC (FEDERACIÓ CATALANA D’ENTITATS CONTRA EL CÁNCER
- FUNDACIÓ KÁLIDA. Barcelona
- FUNDACIÓ ROSES CONTRA EL CÀNCER. Roses
- LLIGA CONTRA EL CÀNCER COMARQUES DE TARRAGONA I TERRES DE L’EBRE. Tarragona
- MielomaCAT
- ONCOLLIGA BARCELONA. Barcelona
- ONCOLLIGA GIRONA. Girona
- ONCOLLIGA COMARQUES DE LLEIDA. Lleida
- ONCOVALLÈS. Vallès Oriental
- OSONA CONTRA EL CÀNCER. Osona
- SUPORT I COMPANYIA. Barcelona
- VILASSAR DE DALT CONTRA EL CÀNCER. Vilassar de Dalt
VALENCIAN COMMUNITY
- AECC (ASOCIACIÓN ESPAÑOLA CONTRA EL CÁNCER). Present is the different provinces and in many municipalities. Contact the nearest branch.
- ASLEUVAL (ASOCIACIÓN DE PACIENTES DE LEUCEMIA, LINFOMA, MIELOMA Y OTRAS ENFERMEDADES DE LA SANGRE DE VALENCIA)
EXTREMADURA
- AECC (ASOCIACIÓN ESPAÑOLA CONTRA EL CÁNCER). Present is the different provinces and in many municipalities. Contact the nearest branch.
- AFAL (AYUDA A FAMILIAS AFECTADAS DE LEUCEMIAS, LINFOMAS; MIELOMAS Y APLASIAS)
- AOEX (ASOCIACIÓN ONCOLÓGICA EXTREMEÑA)
GALICIA
- AECC (ASOCIACIÓN ESPAÑOLA CONTRA EL CÁNCER). Present is the different provinces and in many municipalities. Contact the nearest branch.
- ASOTRAME (ASOCIACIÓN GALLEGA DE AFECTADOS POR TRASPLANTES MEDULARES)
BALEARIC ISLANDS
- ADAA (ASSOCIACIÓ D’AJUDA A L’ACOMPANYAMENT DEL MALALT DE LES ILLES BALEARS)
- AECC (ASOCIACIÓN ESPAÑOLA CONTRA EL CÁNCER). Present is the different provinces and in many municipalities. Contact the nearest branch.
CANARY ISLANDS
- AECC (ASOCIACIÓN ESPAÑOLA CONTRA EL CÁNCER). Present is the different provinces and in many municipalities. Contact the nearest branch.
- AFOL (ASOCIACIÓN DE FAMILIAS ONCOHEMATOLÓGICAS DE LANZAROTE)
- FUNDACIÓN ALEJANDRO DA SILVA
LA RIOJA
- AECC (ASOCIACIÓN ESPAÑOLA CONTRA EL CÁNCER). Present is the different provinces and in many municipalities. Contact the nearest branch.
MADRID
- AECC (ASOCIACIÓN ESPAÑOLA CONTRA EL CÁNCER). Present is the different provinces and in many municipalities. Contact the nearest branch.
- AEAL (ASOCIACIÓN ESPAÑOLA DE LEUCEMIA Y LINFOMA)
- CRIS CONTRA EL CÁNCER
- FUNDACIÓN LEUCEMIA Y LINFOMA
MURCIA
- AECC (ASOCIACIÓN ESPAÑOLA CONTRA EL CÁNCER). Present is the different provinces and in many municipalities. Contact the nearest branch.
NAVARRA
- AECC (ASOCIACIÓN ESPAÑOLA CONTRA EL CÁNCER). Present is the different provinces and in many municipalities. Contact the nearest branch.
BASQUE COUNTRY
- AECC (ASOCIACIÓN ESPAÑOLA CONTRA EL CÁNCER). Present is the different provinces and in many municipalities. Contact the nearest branch.
- PAUSOZ-PAUSO. Bilbao
AUTONOMOUS CITIES OF CEUTA AND MELILLA
- AECC CEUTA (ASOCIACIÓN ESPAÑOLA CONTRA EL CÁNCER)
- AECC MELILLA (ASOCIACIÓN ESPAÑOLA CONTRA EL CÁNCER)
Support and assistance
We also invite you to follow us through our main social media (Facebook, Twitter and Instagram) where we often share testimonies of overcoming this disease.
If you live in Spain, you can also contact us by sending an e-mail to imparables@fcarreras.es so that we can help you get in touch with other people who have overcome this disease.