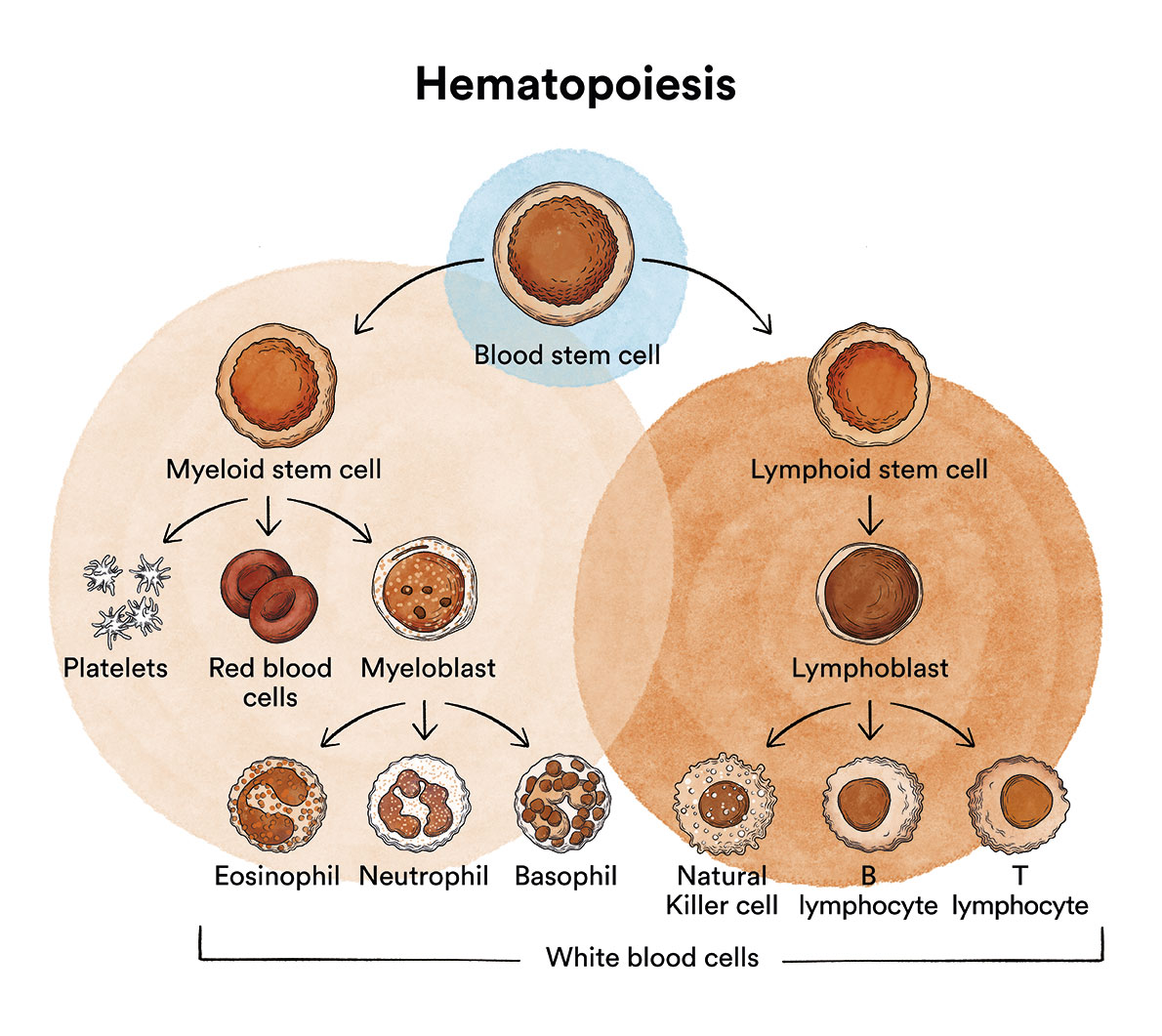
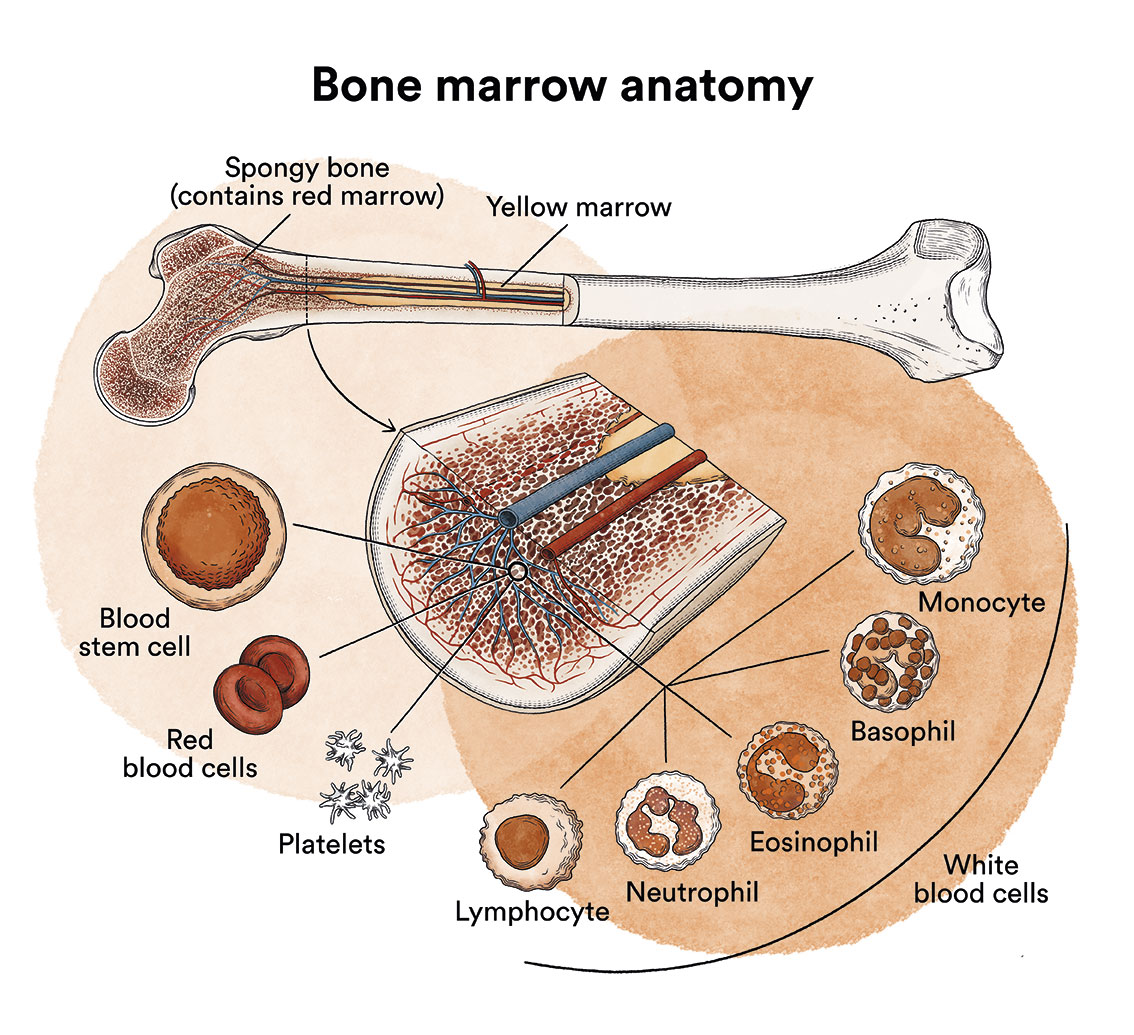
How does bone marrow work and what are the types of blood cells?
Waldeström Macroglobulinemia is a disease that originates in the bone marrow, also called lymphoplasmacytic lymphoma.See section Leukaemia, bone marrow and blood cells.
What is Waldeström Macroglobulinemia and who does it affect?
Waldeström Macroglobulinemia is a disease of the bone marrow, specifically of the plasma cells. Waldeström Macroglobulinemia. Also called lymphoplasmacytic lymphoma, it is a type of cancer characterised by a monoclonal proliferation of B lymphocytes infiltrating lymphoid marrow and organs, with the ability to synthesise and secrete high amounts of monoclonal immunoglobulin M (IgM).
Immunoglobulins (Ig), or antibodies, are substances that circulate in the blood in order to defend the individual by attacking any foreign matter that enters the body. Each Ig consists of two heavy chains (gamma (IgG), alpha (IgA), mu (IgM), delta (IgD) or epsilon (IgE) and two light chains (kappa or delta).
Several diseases are characterised by clonal proliferation of plasma cells. This implies that they produce a single type of light and/or heavy chain (called monoclonal component). These diseases are called monoclonal gammopathies. This is why Waldenström Macroglobulinaemia is classically categorised as a monoclonal gammopathy, but clinically it is more similar to an indolent B-cell non-Hodgkin’s lymphoma (lymphoplasmacytic lymphoma).
Waldenström Macroglobulinaemia is a very rare type of neoplasm. Its incidence in Spain is around 3 cases per million inhabitants per year. It tends to affect predominantly males (70% of patients) of advanced age, with a median age of 71 years, but is not exceptional at younger ages.
What are the causes of Waldenström Macroglobulinaemia?
There is no known direct causative factor for the onset of Waldenström Macroglobulinaemia.
It is not a contagious disease.
What are the symptoms of Waldenström Macroglobulinaemia?
 Waldenström Macroglobulinaemia usually has a chronic and a very slow progression and may remain asymptomatic for years, requiring no treatment.
Waldenström Macroglobulinaemia usually has a chronic and a very slow progression and may remain asymptomatic for years, requiring no treatment.
The main clinical manifestations of symptomatic forms are fatigue, loss of appetite, weight loss, sometimes profuse sweating. The presence of large amounts of IgM can lead to hyperviscosity syndrome. These proteins cause the blood to thicken and this impedes normal blood flow (thick blood) which can lead to neurological (headache, dizziness, confusion, drowsiness), ocular (impaired vision), and cardiac (heart failure) disorders. There may also be haemorrhagic diathesis (predisposition of the organism to bleed abnormally) due to the hyperviscosity and plateletopenia that may be caused by marrow infiltration. Adenopathy (enlarged lymph nodes), splenomegaly (enlarged spleen) or hepatomegaly (enlarged liver) may be observed.
How is Waldeström Macroglobulinaemia diagnosed?
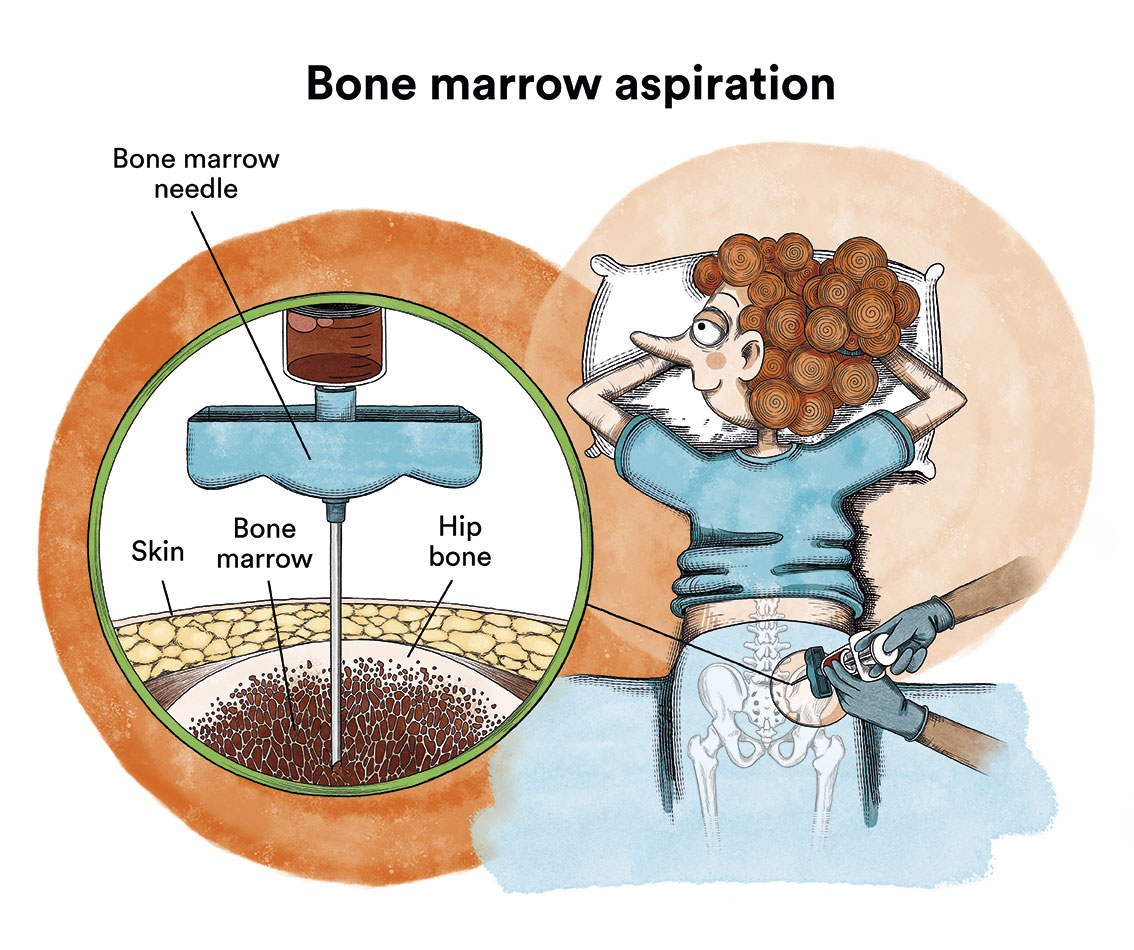
The diagnosis of Waldenström Macroglobulinemia is based on confirmation of lymphomatous infiltration of the bone marrow and demonstration of the monoclonal IgM component in the proteinogram. The study will also require a complete blood count, biochemistry (glycaemia, ionogram, renal profile and liver profile) and coagulation study, cytogenetic and molecular immunophenotypic study (the MYD88 L265P mutation is detected in more than 90% of cases of WM), blood and bone marrow (aspirate and bone marrow biopsy), fundus study to assess hyperviscosity and an abdominal thoracic CT scan if lymphadenopathy or a large tumour mass is suspected. A lymph node biopsy may be required if there are diagnostic doubts and enlarged lymph nodes are accessible.
What is the treatment for Waldenström Macroglobulinemia?
The most incipient or asymptomatic forms of Waldenström Macroglobulinaemia (25% of cases) may not require treatment, and it is sufficient to periodically assess their evolution to determine whether the disease remains stable or progresses.
Treatment is indicated when there is: recurrent fever, night sweats, weight loss, evidence of hyperviscosity syndrome, enlarged lymph nodes or organomegaly, severe anaemia or platelets, coagulation disorders, renal failure.
If treatment is required, it is usually based on a combination of two or three of the following agents: Rituximab (monoclonal antibody against the CD20 receptor specifically presented by neoplastic lymphoid cells), alkylating agents (chlorambucil, bendamustine, cyclophosphamide), Bruton kinase inhibitors (Ibrutinib, also used in monotherapy) and purine analogues (fludarabine and 2CdA). The choice of therapy must be individualised and will depend on the availability of treatments, the patient’s comorbidities and genetic characteristics of the disease (MYD88 and CXCR4 mutations). Treatment of relapses will depend on the regimen used as first line, with ibrutinib being one of the most frequently used (if not previously received).
Seventy-five percent of patients will have excellent responses to such treatments that can last from 6 months to 8 years.
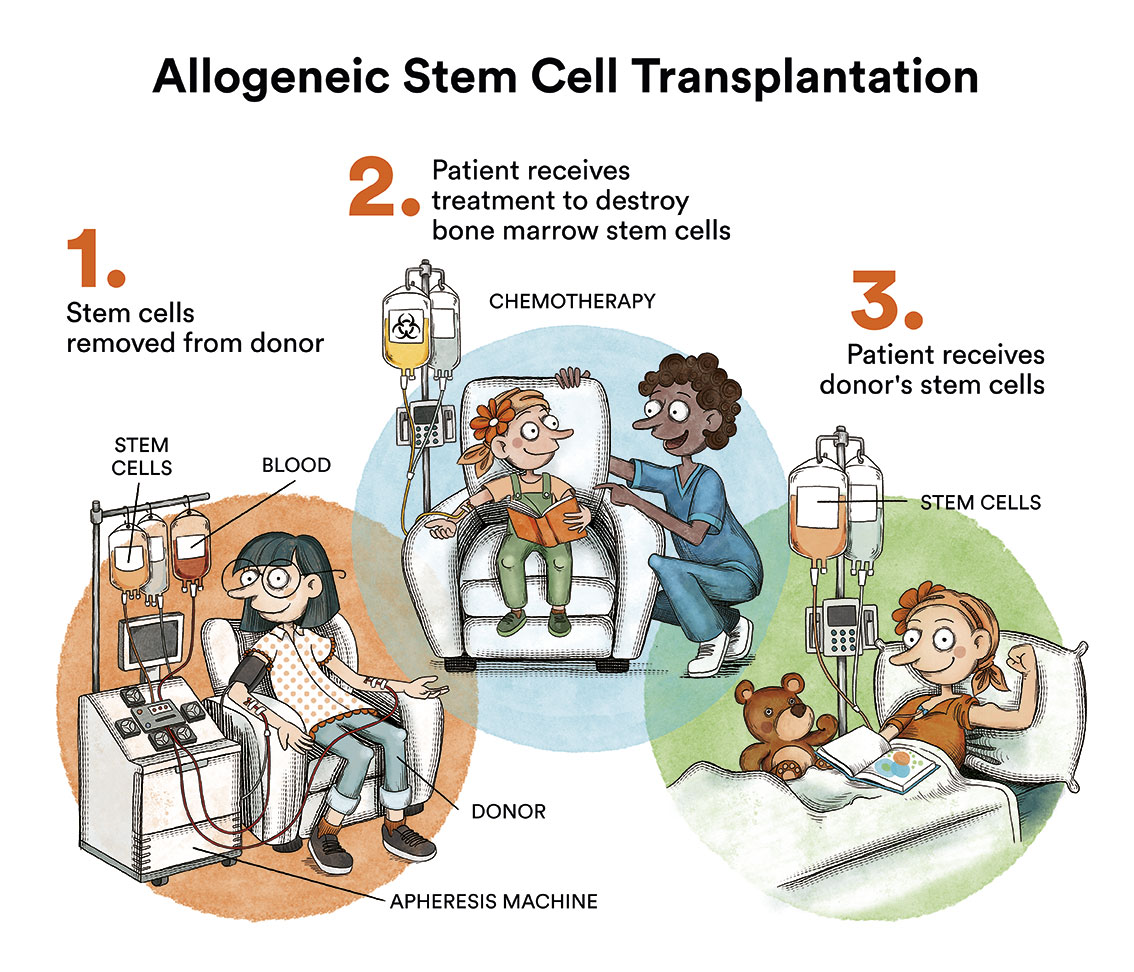
The only treatment for Waldenström Macroglobulinemia with curative possibilities is allogeneic haematopoietic transplantation. Unfortunately, the advanced age of most patients and the high toxicity of the procedure mean that it is rarely used.
In cases with hyperviscosity symptoms, plasmapheresis is indicated until symptoms disappear. This method allows the blood to be completely removed from the body and the red and white blood cells to be separated from the plasma. The blood cells are returned to the patient and the thickened plasma is replaced with normal plasma.
What is the prognosis for patients with Waldenström Macroglobulinemia?
 The prognosis for patients with Waldenström Macroglobulinaemia depends on several factors, including the age of the patient, the speed of disease progression and the response to treatment. Some patients may have stable or slowly progressive disease, and may live for many years. Other patients may have a rapidly progressive form of Waldenström Macroglobulinaemia. 60% of patients are still alive 10 years after diagnosis. About 10-15% of patients have a disease that develops into aggressive non-Hodgkin’s lymphoma (link to non-Hodgkin’s lymphoma) and should be treated as such.
The prognosis for patients with Waldenström Macroglobulinaemia depends on several factors, including the age of the patient, the speed of disease progression and the response to treatment. Some patients may have stable or slowly progressive disease, and may live for many years. Other patients may have a rapidly progressive form of Waldenström Macroglobulinaemia. 60% of patients are still alive 10 years after diagnosis. About 10-15% of patients have a disease that develops into aggressive non-Hodgkin’s lymphoma (link to non-Hodgkin’s lymphoma) and should be treated as such.
Links of interest concerning medical issues relating to Waldenström Macroglobulinemia
What Is Waldenstrom Macroglobulinemia? American Cancer Society
Waldenström macroglobulinaemia (WM). Blood Cancer UK
Waldenström macroglobulinemia (WM). Leukemia & Lymphoma Foundation
Links of interest on other topics related to Waldeström Macroglobulinemia
TESTIMONIAL MATERIALS
You can order the booklets in paper format for free delivery in Spain by e-mail: imparables@fcarreras.es
BONE MARROW TRANSPLANT
- Bone Marrow Transplant Guide. Josep Carreras Foundation (content in Spanish)
- What is HLA and how does it work? Josep Carreras Foundation (content in Spanish)
- Graft-versus-Host Disease. Josep Carreras Foundation (content in Spanish)
- History of Bone Marrow Transplantation. Josep Carreras Foundation (content in Spanish)
- How is the search for an anonymous donor conducted? Josep Carreras Foundation (content in Spanish)
FOOD
- How to maintain a healthy diet during treatment? Josep Carreras Foundation (content in Spanish)
- Nutrition guide. Leukemia & Lymphoma Society
OTHER
- Ideas on what to take with me to the isolation chamber. Josep Carreras Leukaemia Foundation (content in Spanish)
- Travel tips for people with cancer. Josep Carreras Leukaemia Foundation (content in Spanish)
- Physiotherapy manual for haematological and transplant patients. Josep Carreras Leukaemia Foundation (content in Spanish)
- Prevention and treatment of oral mucositis. Josep Carreras Leukaemia Foundation (content in Spanish)
- Oral hygiene in oncohaematological patients. Josep Carreras Leukaemia Foundation (content in Spanish)
- Fertility manual: Suffering from blood cancer and becoming a parent. Josep Carreras Leukaemia Foundation (content in Spanish)
- Skin care in the oncohaematological patient. Josep Carreras Leukaemia Foundation (content in Spanish)
- Aesthetic Oncology Manual. Josep Carreras Leukaemia Foundation (content in Spanish)
- Leukaemia and sexuality. Josep Carreras Leukaemia Foundation (content in Spanish)
- 7 ways to wear a scarf. Josep Carreras Leukaemia Foundation (content in Spanish)
Links of interest: local/provincial or state entities that can provide you with resources and services specialised in leukaemia or cancer patients:
In Spain there is a large network of associations for haematological cancer patients that, in many cases, can inform you, advise you and even carry out certain procedures. These are the contacts of some of them by Autonomous Communities:
All these organisations are external to the Josep Carreras Foundation.
STATE
- CEMMP (Comunidad Española de Pacientes de Mieloma Múltiple)
- AEAL (ASOCIACIÓN ESPAÑOLA DE AFECTADOS POR LINFOMA, MIELOMA y LEUCEMIA)
- AECC (ASOCIACIÓN ESPAÑOLA CONTRA EL CÁNCER). Present is the different provinces and in many municipalities. Contact with the nearest branch or call 900 100 036 (24h).
- AELCLES (Agrupación Española contra la Leucemia y Enfermedades de la Sangre)
- Josep Carreras Leukaemia Foundation
- FUNDACIÓN SANDRA IBARRA
- GEPAC (GRUPO ESPAÑOL DE PACIENTES CON CÁNCER)
- MPN España (Asociación de Afectados Por Neoplasias Mieloproliferativas Crónicas)
ANDALUCÍA
- AECC (ASOCIACIÓN ESPAÑOLA CONTRA EL CÁNCER). Present is the different provinces and in many municipalities. Contact the nearest branch.
- ALUSVI (ASOCIACIÓN LUCHA Y SONRÍE POR LA VIDA). Sevilla
- APOLEU (ASOCIACIÓN DE APOYO A PACIENTES Y FAMILIARES DE LEUCEMIA). Cádiz
ARAGÓN
- AECC (ASOCIACIÓN ESPAÑOLA CONTRA EL CÁNCER). Present is the different provinces and in many municipalities. Contact the nearest branch.
- ASPHER (ASOCIACIÓN DE PACIENTES DE ENFERMEDADES HEMATOLÓGICAS RARAS DE ARAGÓN)
- DONA MÉDULA ARAGÓN
ASTURIAS
- AECC (ASOCIACIÓN ESPAÑOLA CONTRA EL CÁNCER). Present is the different provinces and in many municipalities. Contact the nearest branch.
- ASTHEHA (ASOCIACIÓN DE TRASPLANTADOS HEMATOPOYÉTICOS Y ENFERMOS HEMATOLÓGICOS DE ASTURIAS)
CANTABRIA
- AECC (ASOCIACIÓN ESPAÑOLA CONTRA EL CÁNCER). Present is the different provinces and in many municipalities. Contact the nearest branch.
CASTILLA LA MANCHA
- AECC (ASOCIACIÓN ESPAÑOLA CONTRA EL CÁNCER). Present is the different provinces and in many municipalities. Contact the nearest branch.
CASTILLA LEÓN
- ABACES (ASOCIACIÓN BERCIANA DE AYUDA CONTRA LAS ENFERMEDADES DE LA SANGRE)
- AECC (ASOCIACIÓN ESPAÑOLA CONTRA EL CÁNCER). Present is the different provinces and in many municipalities. Contact the nearest branch.
- ALCLES (ASOCIACIÓN LEONESA CON LAS ENFERMEDADES DE LA SANGRE). León.
- ASCOL (ASOCIACIÓN CONTRA LA LEUCEMIA Y ENFERMEDADES DE LA SANGRE). Salamanca.
CATALUÑA
- ASSOCIACIÓ FÈNIX. Solsona
- FECEC (FEDERACIÓ CATALANA D’ENTITATS CONTRA EL CÁNCER
- FUNDACIÓ KÁLIDA. Barcelona
- FUNDACIÓ ROSES CONTRA EL CÀNCER. Roses
- LLIGA CONTRA EL CÀNCER COMARQUES DE TARRAGONA I TERRES DE L’EBRE. Tarragona
- MielomaCAT
- ONCOLLIGA BARCELONA. Barcelona
- ONCOLLIGA GIRONA. Girona
- ONCOLLIGA COMARQUES DE LLEIDA. Lleida
- ONCOVALLÈS. Vallès Oriental
- OSONA CONTRA EL CÀNCER. Osona
- SUPORT I COMPANYIA. Barcelona
- VILASSAR DE DALT CONTRA EL CÀNCER. Vilassar de Dalt
VALENCIAN COMMUNITY
- AECC (ASOCIACIÓN ESPAÑOLA CONTRA EL CÁNCER). Present is the different provinces and in many municipalities. Contact the nearest branch.
- ASLEUVAL (ASOCIACIÓN DE PACIENTES DE LEUCEMIA, LINFOMA, MIELOMA Y OTRAS ENFERMEDADES DE LA SANGRE DE VALENCIA)
EXTREMADURA
- AECC (ASOCIACIÓN ESPAÑOLA CONTRA EL CÁNCER). Present is the different provinces and in many municipalities. Contact the nearest branch.
- AFAL (AYUDA A FAMILIAS AFECTADAS DE LEUCEMIAS, LINFOMAS; MIELOMAS Y APLASIAS)
- AOEX (ASOCIACIÓN ONCOLÓGICA EXTREMEÑA)
GALICIA
- AECC (ASOCIACIÓN ESPAÑOLA CONTRA EL CÁNCER). Present is the different provinces and in many municipalities. Contact the nearest branch.
- ASOTRAME (ASOCIACIÓN GALLEGA DE AFECTADOS POR TRASPLANTES MEDULARES)
BALEARIC ISLANDS
- ADAA (ASSOCIACIÓ D’AJUDA A L’ACOMPANYAMENT DEL MALALT DE LES ILLES BALEARS)
- AECC (ASOCIACIÓN ESPAÑOLA CONTRA EL CÁNCER). Present is the different provinces and in many municipalities. Contact the nearest branch.
CANARY ISLANDS
- AECC (ASOCIACIÓN ESPAÑOLA CONTRA EL CÁNCER). Present is the different provinces and in many municipalities. Contact the nearest branch.
- AFOL (ASOCIACIÓN DE FAMILIAS ONCOHEMATOLÓGICAS DE LANZAROTE)
- FUNDACIÓN ALEJANDRO DA SILVA
LA RIOJA
- AECC (ASOCIACIÓN ESPAÑOLA CONTRA EL CÁNCER). Present is the different provinces and in many municipalities. Contact the nearest branch.
MADRID
- AECC (ASOCIACIÓN ESPAÑOLA CONTRA EL CÁNCER). Present is the different provinces and in many municipalities. Contact the nearest branch.
- AEAL (ASOCIACIÓN ESPAÑOLA DE LEUCEMIA Y LINFOMA)
- CRIS CONTRA EL CÁNCER
- FUNDACIÓN LEUCEMIA Y LINFOMA
MURCIA
- AECC (ASOCIACIÓN ESPAÑOLA CONTRA EL CÁNCER). Present is the different provinces and in many municipalities. Contact the nearest branch.
NAVARRA
- AECC (ASOCIACIÓN ESPAÑOLA CONTRA EL CÁNCER). Present is the different provinces and in many municipalities. Contact the nearest branch.
BASQUE COUNTRY
- AECC (ASOCIACIÓN ESPAÑOLA CONTRA EL CÁNCER). Present is the different provinces and in many municipalities. Contact the nearest branch.
- PAUSOZ-PAUSO. Bilbao
AUTONOMOUS CITIES OF CEUTA AND MELILLA
- AECC CEUTA (ASOCIACIÓN ESPAÑOLA CONTRA EL CÁNCER)
- AECC MELILLA (ASOCIACIÓN ESPAÑOLA CONTRA EL CÁNCER)
Support and assistance
We also invite you to follow us through our main social media (Facebook, Twitter and Instagram) where we often share testimonies of overcoming this disease.
If you live in Spain, you can also contact us by sending an e-mail to imparables@fcarreras.es so that we can help you get in touch with other people who have overcome this disease.